Early Embryonic Death
By Jonathan F Pycock, BVetMed, PhD, DESM, MRCVS, RCVS Specialist in Equine Reproduction
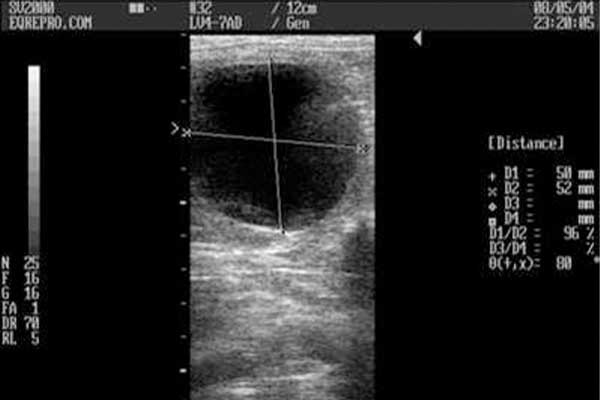
Fig. 1

Fig. 2
For all horse breeders, it is important to realize that not every mare will give birth to a live foal. Failure of the pregnancy can occur at any stage starting from the fertilization of the oocyte or egg. The oocyte develops in the fluid-filled follicle (Figure One). When it is mature, the oocyte is shed from the follicle into the fallopian tube. This is called ovulation. The fallopian tubes, or oviducts, stretch from the uterus to the ovaries. If the mare has been bred by a stallion or inseminated in the last two or three days, the fallopian tubes should contain sperm (Figure Two). A sperm will burrow into an oocyte and fertilize it to produce the early embryo.
In the mare, fertilization occurs in the fallopian tube and can take place through either natural or artificial insemination. It is a unique event that brings the genetic material of the parents together. It also is a very complex process in terms of both timing and management. Sperm normally live only two or three days in the fallopian tube, so the mare should not be bred too early in estrus or the sperm could be dead before the oocyte arrives in the fallopian tube. You might wonder how the sperm and oocyte ever manage to meet, but statistics show that pregnancy rates average out at 70% by the end of the season.
The fertilized embryo remains in the oviduct for five to six days. After that time, it leaves the oviduct and enters the uterus. The equine oviduct appears to have the unique ability to retain unfertilized ova. This discovery was made as long ago as 1966 and has been confirmed by many subsequent studies. The mechanism remains unclear to this day.
The next stage in the reproductive process is gestation, which begins when the oocyte is fertilized and ends at birth. During that time, the fetus develops and grows to a state where the newborn foal can survive in the outside world. There are hormonal changes during pregnancy; in particular the hormone group progestins continue to be produced.
For the first 14 days of pregnancy, the hormones produced by the mare do not differ from those of the non-pregnant mare when she is out of season; i.e., in the diestrus or luteal phase of the heat cycle. You remember that in the non-pregnant mare, a hormone called prostaglandin is released about Day 14. That prostaglandin destroys the progesterone-producing corpus luteum (formed from the tissues of the burst follicle after ovulation) and causes the mare to come back into heat (estrus). In the pregnant mare, the release of prostaglandin has to be stopped. It is not yet clear exactly how this happens, but the early mobility of the pregnancy is important in the mechanism. In the pregnant mare, the corpus luteum (CL) persists and continues to produce the hormone progesterone, which prevents the mare from coming back into heat.
The early pregnancy, called the embryonic vesicle, moves around the inside of the uterus for about 10 days. It eventually becomes stationary on about the 16th day after ovulation occurred. This termination of movement is called fixation and apparently is caused by the increasing uterine tone combined with the increasing size of the pregnancy. The pregnancy normally is fixed at the base of either the left or the right uterine horn. Up until that point, the pregnancy has been spherical in shape. When it fixes, it assumes an irregular shape associated with the loss of its protective and capsule; the vesicle then enlarges longitudinally whilst the cross sectional area enlarges more slowly.
An early diagnosis of pregnancy is important because mares carrying foals need careful management. The foal potentially is very valuable in economic or personal terms for most breeders. The most common method of pregnancy diagnosis used in the horse breeding industry is ultrasound examination of the uterus. The early fluid-filled pregnancy can be imaged as a black disc. Its growth can be monitored and appropriate action taken if there are twin pregnancies or signs of the pregnancy’s being lost. Pregnancy failure is a source of major economic loss to the horse industry.
A unique feature of pregnancy in the horse is the endometrial cups. They are distinctive, irregularly shaped areas that develop in a ring at the base of the pregnant horn of the uterus. The cups produce a hormone called equine chorionic gonadotrophin (eCG), which appears in the mare’s bloodstream around Day 35 of pregnancy. A traditional name for this hormone is pregnant mare’s serum gonadotrophin. This hormone can persist in the bloodstream for as long as 150 days. It has a major role to play in early pregnancy in stimulating the ovaries to produce more progesterone, thereby preventing her from coming back into heat.
Progesterone stops the mare from coming back into heat, and in the pregnant mare the CL is not destroyed around Day 14/15/16, but persists and continues to produce progesterone. This is called the maternal recognition of pregnancy. Maternal recognition of pregnancy is the process whereby destruction of the CL is prevented by the presence of the conceptus. This prolongs progesterone secretion for the maintenance of pregnancy. The mechanism by which the equine conceptus signals its presence to the mare to prevent destruction of the CL is unknown. The first step in the maternal recognition of pregnancy signaling mechanism must involve an interaction with the lining of the uterus (termed the endometrium).
Endometrial secretions are important in the maintenance of early pregnancy in the mare. This is supported by the finding that the mare has an unusually rich supply of tightly coiled secretory glands in her uterine wall that produce large amounts of a protein-rich secretion during the luteal phase of the estrous cycle and early pregnancy. The constituents of this early secretion have not been well characterized in the mare.
Movement of the embryonic vesicle throughout the uterus until about day 16 post-ovulation is thought to be important for the conceptus to “signal” to the dam that pregnancy has occurred, thereby preventing luteolysis (degeneration of the corpus luteum).
The critical time for maternal recognition of pregnancy, in order to prevent luteolysis of the primary CL and subsequent loss of the pregnancy, is thought to be 14-16 days after ovulation in the mare. Conditions that prevent the conceptus from migrating throughout the uterus (e.g. blocked uterine horn) interfere with maternal recognition of pregnancy, resulting in failure to prevent endometrial production and release of prostaglandin. That will allow the mare to return to estrus in spite of conceiving.
The eCG is responsible for the continued maintenance and development of the CL beyond Day 35. In addition, eCG can cause further CLs to form. These are known as secondary or accessory CLs. If pregnancy loss occurs before eCG is produced (in the period up to Day 35 of pregnancy), the mare will come back into heat. Once the mare has started to produce eCG, she usually cannot be bred again successfully that year.
Pregnancy Development: Definitions
The embryo is the name given to the new life developing in the uterus before the various body parts are recognizable. Once all the organs have been formed, the future foal is called a fetus. The organs all are formed and the foal is essentially a miniature replica of a term foal from about 40 days in the mare.
There are critical periods of development of the pregnancy: early embryonic death occurs before 40 days of gestation and perhaps even before the dam recognizes she is pregnant around days 14 to 16 of pregnancy. When loss occurs early in pregnancy, the term resorption may be used. In such cases, the dead embryo or fetus is not found. Particularly if loss occurs after about 30 days, the mare might not return to estrus for some time, entering a state of false pregnancy.
Early fetal death occurs before 150 days of gestation; thus, late fetal death occurs afterward. Abortion refers to loss of the fetus and its membranes before Day 300 of gestation. The fetus at that stage, even with intensive care, is very unlikely to survive. Prematurity is the term used to describe a foal born between Days 300 and 320. Such foals usually can survive with good nursing and health care. A stillbirth usually refers to a dead foal produced after 300 days of pregnancy.
Slipping is a term used to describe the abortion of a foal. The term commonly is used when the actual fetal foal is found in the field or stable.
However, these definitions all are somewhat arbitrary and fetal death, resorption, and slipping all have more or less the same meaning as abortion.
This article will focus on the period of early pregnancy loss, i.e., early embryonic death (EED).
Incidence Of Embryonic Death
In normal fertile mares, the fertilization rate is greater than 90%, which is comparable with other domestic species. There are estimates of the EED rate at between 5% and 24%. In subfertile mares, the rate is higher. The differences in the estimates are due to varying methods of pregnancy detection, and the animals studied.
The period of greatest embryonic death in subfertile mares occurs in the interval before pregnancy can be easily detected with ultrasound (Day 11), particularly at the time the embryo enters the uterus. Between Days 14 and 40, the rate of embryonic death varies between 10% and 17%.
Causes Of Early Embryonic Death
EED is multifactorial, in which external factors such as the environment and management as well as pathophysiological factors are involved. However, the evidence for many of these associations are anecdotal and frequently contradictory. This might be because few cases of EED have been able to be studied in detail, which could have allowed their causes to be established.
External Factors
External factors include stress, nutrition, season of the year, climate, sire effects, and rectal palpation.
Maternal stress due to severe pain, malnutrition, and transport has been implicated as a cause of EED. Frequently, mares are transported at various stages of pregnancy. Recent research failed to demonstrate any difference in pregnancy rates between transported and non-transported mares. Transporting pregnant mares home from stud a distance of 300 miles (500 km) in less than nine hours of traveling time can be stressful, but should not result in embryonic death. If a longer journey is necessary, the journey should be broken after eight hours.
Waiting until the fifth week of pregnancy, or later, to transport broodmares might be advisable when critical events such as descent of the embryo into the uterus and transition from the yolk sac to the chorioallantoic placentation have occurred. The common practice of transporting mares to stud for breeding and returning home the same day should not be detrimental to their fertility as long as the transport is safe and comfortable.
Far from being avoided, regular exercise is important during pregnancy, although during the latter half, forced exercise should be decreased, and during early pregnancy ambient weather conditions should be considered. Recent research (2007) demonstrated a lower embryo recovery rate from mares exercised daily for 30 min under average ambient conditions of >30°C and >50% humidity when compared to non-exercised mares (34% vs. 63%). This suggests that an increased core temperature brought about by exercise under such ambient weather conditions during the early embryonic period may negatively impact embryo survival.
There is a limited amount of evidence to suggest that there are significant differences in the incidence of EED among stallions. Subfertile stallions in particular might be more likely to have a high likelihood of EED. However, a large study conducted recently found no differences among stallions in rates of EED.
Rectal palpation and ultrasound examinations should be considered safe procedures when performed correctly, and recent evidence gives no indication that ultrasound examination is detrimental to the embryo.
Mare Reproductive Loss Syndrome (MRLS): First and last trimester fetal losses have been observed in recent years in large number of mares in Kentucky, particularly in 2001 and 2002. Not only were pregnancy losses involved, but other systemic problems such as pericarditis and in some cases unilateral uveitis were observed in the mares. Although early pregnancy loss was most significant, there was also a higher incidence of later term pregnancy loss, with mares aborting with little or no classical indication of impending parturition and a high incidence of premature placental separation. The term mare reproductive loss syndrome (MRLS) was given to the condition. Although much remains to be learned about the syndrome, involvement of the eastern tent caterpillar seems to be directly associated with the syndrome.
Maternal Factors
A number of abnormal maternal factors, including hormone deficiencies and imbalances, uterine environment, age, and lactation have been implicated.
Hormonal Deficiencies And Imbalances
Progesterone is critical for the maintenance of pregnancy in mares. A deficiency of progesterone often has been suggested as a cause of EED. The only source of progesterone during the embryonic period is the primary CL. On the assumption that, in mares which suffer EED the CL might be in some way deficient in producing progesterone, many mares are given exogenous progesterone or progestogens in an attempt to prevent loss from occurring. The rationale for this widespread practice is questionable, although primary luteal insufficiency as a cause of EED has been reported.

Fig. 3
Progesterone supplementation is popular among some veterinarians and breeding farms, while others are skeptical of any benefit. Many dosage regimens do not effectively elevate or maintain plasma progesterone levels. Withdrawal of supplementary progesterone therapy during mid-gestation might leave the clinician open to criticism if the mare subsequently aborts. In the author’s opinion, progesterone therapy is most appropriate in mares which have uterine edema (Figure Three) and an indistinct CL at the time of the first ultrasonographic examination for pregnancy (ideally 14 to 15 days after ovulation). These pregnancies usually are lost within a few days, but some can be successfully “saved” by exogenous progesterone and the pregnancy carry normally through to term. Progesterone in oil (100 mg ) or altrenogest (35 mg; Regumate) are given daily until a CL is obvious on ultrasound examination and all uterine edema has disappeared. Biorelease formulations of both progesterone and altrenogest are available (BET Pharmacy, Lexington, KY USA) which do not require daily treatment but provide a sustained release over a period of days.
A single injection of 40 micrograms of the gonadotrophin-releasing hormone (GnRH) analog buserelin (Receptal) also has been shown to reduce the incidence of EED when given 10 days after ovulation. The mechanism of action for this improvement in the pregnancy rate using buserelin is not known. It is essential that there is a thorough investigation of the effects of GnRH and its analogs to allow for any possible advantage for its use. There is a need for further research to confirm the repeatability of the data of the study indicating an increase in pregnancy maintenance rate following buserelin treatment. It is possible that treatment with buserelin in late diestrus before the occurrence of a luteolytic signal might prevent luteal regression in mares in which the embryonic vesicle alone is not capable of blocking luteolysis.
Uterine Environment
An abnormal uterine environment is detrimental to embryonic survival. Acute endometritis can result in EED by inducing premature luteolysis or because of its direct effect on the embryo.
Severe periglandular fibrosis of the uterine glands might reduce the chances of embryo survival. Not only is this a response to persistent endometritis, but it also increases with age. This is one of the reasons for the reduced fertility of mares more than 12 years of age. Despite similar fertilization rates, detected pregnancy rates are on average 33% lower. This reported increase in the rate of EED with advancing maternal age also could be due to defects in the fertilization process.
Foal Heat Breeding
The mare normally resumes cyclical ovarian activity very shortly after parturition so that she sometimes is bred as early as seven to 10 days postpartum (at the foal heat). An advantage of breeding at the first estrus postpartum is that the foaling to conception interval is significantly shorter. There is conflicting evidence about the level of embryonic death if fertilization occurs at this time, with some studies showing a higher rate and others no effect. In any case, with the advent of ultrasound to detect EED more readily than before, mares which have lost an early pregnancy can be recognized more quickly and bred again.
The reason for the apparent decreased fertility in mares mated at the foal heat is the hostile uterine environment due to delayed uterine involution or persistent endometritis. However, pregnancy rates clearly are influenced by how strict the selection criteria are for mating at the foal heat. Traditionally, such factors as a normal foaling, placental expulsion, minimal vaginal bruising, and absence of infection have been used. Endometrial cytology and ultrasonic scanning of the genital tract of each mare might be more reliable methods on which to base a decision.
Lactation
More pregnancy failures are detected in lactating than non-lactating (maiden or barren) mares. This failure in lactating mares also increases with the age of the mare. Lactating mares also might be more susceptible to detrimental effects of poor diet.
Embryonic Factors
Genetic and embryonic abnormalities are important to consider in relation to embryonic death. In other species, genetic factors are known to contribute to EED, and so might be involved in EED of the horse. In many cases, these genetic factors are not inherited from the parents, but arise from defective gametes (the egg and the sperm) perhaps due to aging of the gametes. This can occur when mares are bred too early in estrus and the sperm are several days old before fertilization. Similarly, if mares are bred after ovulation, the oocyte (which seems not to live as long as the sperm once it has been released) might have aged and be defective.
Embryos recovered from subfertile mares are smaller and have more morphological defects than embryos from fertile mares. However, this could be due to an abnormal uterine environment.
Twin Pregnancy
Early embryonic losses in multiple pregnancies are greater than for single pregnancies. Double ovulations increase the likelihood of twin conception. There is considerable breed variation in the incidence of multiple ovulation. The Thoroughbred has a very high rate of double ovulation, with the author’s data from the last two breeding seasons indicating an incidence of around 34%. This is much higher than previously reported studies.
Pregnancy Diagnosis
Early pregnancy diagnosis is essential for management and husbandry reasons:
Pregnant mares should be managed differently from non-pregnant mares and have further examinations to monitor the development of the pregnancy, confirm the absence of twin pregnancies, and monitor for early embryonic or fetal death. Twin pregnancies are bad news in the mare and should be avoided. If a twin pregnancy is diagnosed early enough, the situation can be rectified. In order to detect pregnancy loss in the mare, it is important to be familiar with the signs of early pregnancy. Only by a thorough understanding of the normal features of the equine pregnancy can deviations from the normal be interpreted accurately.
There are three main methods used to diagnose pregnancy:
- Assessing the mare’s behavior by daily teasing.
- Measuring hormone levels in a blood sample from the mare.
- Conducting a clinical examination by a veterinarian.
The first two described only have limited application, and essentially the only method used is a clinical examination using ultrasound.
Daily Teasing
Assessing the pregnant mare’s behavior by daily teasing from Day 12 to 24 should show aggressive rejection of the male. Teasing is a very important part of routine stud farm gynecological management, but mares vary enormously in their displays of signs of estrus. To some extent, this is influenced by the technique used to tease the mare. Some mares will display estrous signs readily, even to other mares or people. Estrous signs occasionally can be seen in mares in diestrus and late pregnancy due to vulval irritation. Other mares will not show estrous signs at all. Mares bred for the first time (maiden mares) or mares with a foal at foot are likely candidates for failing to show estrous behavior at teasing. Therefore, a significant number of mares either do not exhibit signs of estrous, or are slow to show detectable signs using standard teasing methods despite the fact that they are in estrus. This is called silent estrus. The incidence of silent estrus is thought to be approximately 6%. It is thought to have a higher incidence in maiden mares early in the breeding season and in mares with a young foal at foot.
Other factors which affect estrous behavior include being at pasture with very dominant mares, and stallion preferences. Mares which are in training and have been treated with anabolic steroids might be more likely to suffer from the condition due to androgenization (producing masculine characteristics).
To confuse matters further, some mares might have a defect in their systems that prevents the CL from disappearing on or around the 15th day. As a result, enough progesterone is produced to keep the mare out of heat even though she is not pregnant. The same is true for mares which undergo early embryonic death after Day 15 and prolong the lifespan of the primary CL.
Therefore, additional methods of pregnancy diagnosis are required.
Measuring Hormone Levels
The second method of pregnancy diagnosis is by measuring hormone concentrations in a blood (or urine) sample from the mare. This approach can be used where there are inadequate examination facilities, uncooperative animals, miniature horses, or clinician inexperience. There are three hormones which, if present, can indicate pregnancy. They are as follows:
Progesterone
Progesterone prevents the mare from going into heat. In the pregnant mare, the CL is not destroyed and continues to produce progesterone. Therefore, if you discover high progesterone levels in a mare 18 to 20 days after breeding or insemination, you could assume that the mare is pregnant. However, some mares which are not pregnant do not get rid of the CL and progesterone levels can be high in those mares. Also in cases of early embryonic death, false positive results can be obtained.
eCG
There are detectable concentrations of eCG in the blood from approximately 40 days after ovulation. These concentrations usually persist until 80-120 days after ovulation, when a maternal immunological reaction means they no longer function. The amount of eCG produced varies enormously from mare to mare. False positive results in the test are seen in mares in which the pregnancy fails after the endometrial cups have formed and continue to produce eCG. False negative results can be seen if sampling is at an incorrect time and in some mares which can be negative for eCG as early as 70 days after ovulation.
Estrogen
Later in the pregnancy, levels of the hormone estrogen can be measured in the blood and urine. The estrogens come from the feto-placental unit, especially the fetal gonads (which are very large during the latter stages of pregnancy). Although small amounts of estrogen are produced by the follicles on the ovaries, these amounts are too small to interfere with the assay. High estrogen levels from 100 days to approximately 2 weeks prior to term are a non-specific guide that the mare is in foal.
Clinical Examination
The third method of pregnancy diagnosis is a clinical examination by a veterinarian, who performs rectal palpation and ultrasound of the internal organs. With the introduction of diagnostic ultrasonography, accurate pregnancy diagnosis at an early stage of the pregnancy is possible. It is the most reliable method of detection because there are characteristic changes in the feel of the pregnant uterus and also in its appearance on ultrasound scan. The uterus swells due to the presence of a developing pregnancy and this can be monitored by rectal examination.
- By about 25 days the swelling is the size of a golf ball.
- By 30 days the pregnancy is the size of a billiard ball.
- By 40 days, it is the size of a tennis ball.
Between Days 60 to 100, the uterus is low within the abdomen and the fetus usually cannot be palpated; however, from four to five months and onward, it can be examined by touch.
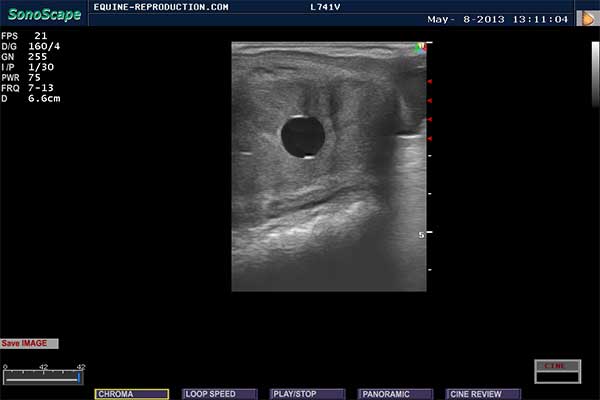
Fig. 4 – day 12
Today, the most common method of diagnosing pregnancy is by ultrasound examination. An ultrasound scan can detect pregnancy as early as 9 days after ovulation, although detection by 11 days at the earliest is more common. In addition, the scanner will detect twin pregnancies and can check that the pregnancy is developing and growing normally. By using ultrasound examination, the equine pregnancy can first be reliably detected at Day 12, when it is seen on the scanner as a perfectly round, black disc with a diameter of 5 to 8 mm (Figure Four). Remember that the sound beams from the ultrasound scanner pass through fluid-filled structures, making them appear black on the screen. Note the two hyperechoic short lines on the dorsal and ventral borders of the conceptus known as specular reflections. While they might aid location of the early embryonic vesicle, they are not indicative of pregnancy but are a physical phenomenon arising from the reflection of the ultrasound beam; cysts tend to cause non-specular reflections.
Mares usually are not scanned as early as Day 12 because it is possible to miss the pregnancy if scanning conditions are not ideal. If there was an ovulation one or two days after the first ovulation, any pregnancy arising from this later ovulation would be too small to be detected. The pregnancy is highly mobile at that stage. Since the pregnancy might be in either the uterine horn or in the uterine body, the entire uterus must be examined thoroughly.
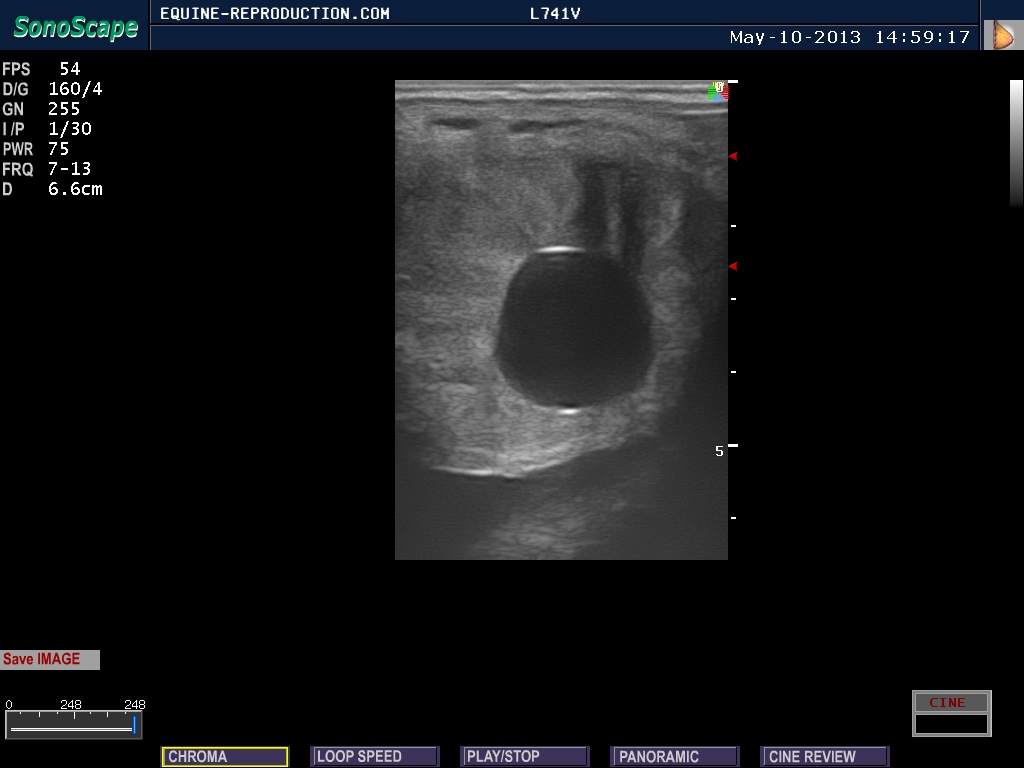
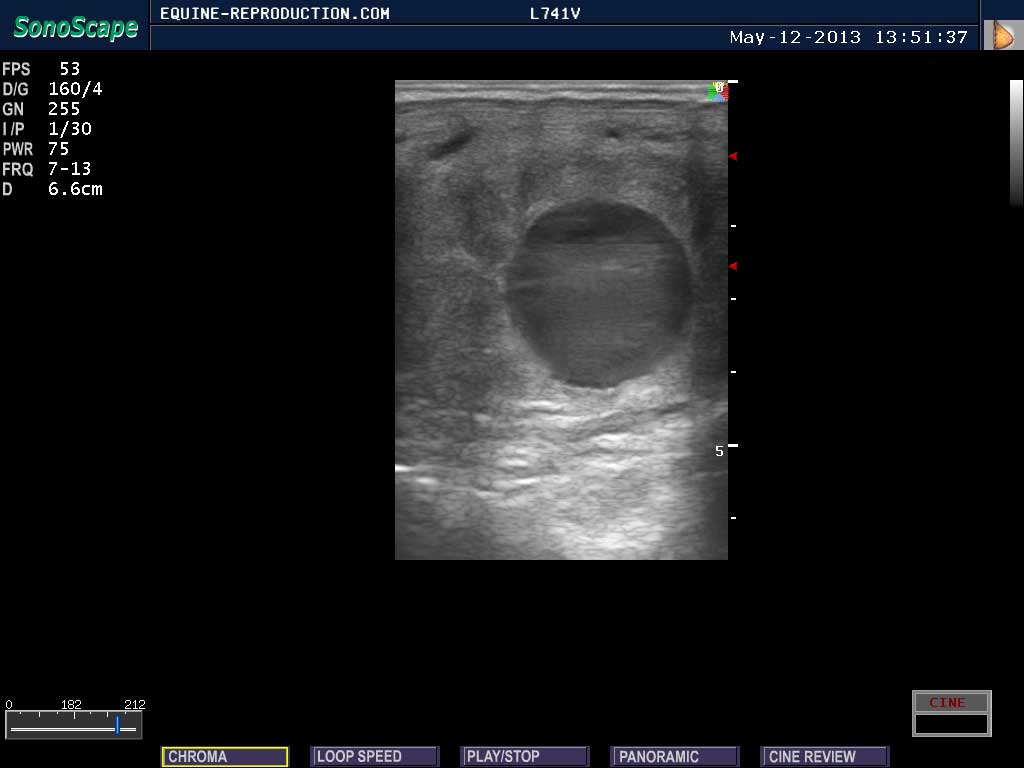
Fig. 5 – day 14
The first scan for pregnancy usually is performed 14 to 15 days after ovulation. The 14 day conceptus is 13 to 18 mm in size and, in this image, lies centrally in the uterine body (Figure Five). Note the spherical shape and increase in size over the Day 11 pregnancy. The embryonic vesicle grows at a rate of approximately 3.5 mm/day at this early stage of pregnancy and remains highly mobile, making thorough examination of all parts of the uterus important. In the event of twin pregnancies, both vesicles can often be seen at 14 days, even if the second twin arose from a later ovulation. This fact, together with the mobility and relatively small size of the concepti, make 14 to 15 days the optimal stage of pregnancy to diagnose twins and crush one.

Fig. 6 – Twins?
Although pregnancy diagnosis is highly accurate even at this early stage, it is important to be aware of the possible confusion caused by uterine cysts and the presence of single or multiple concepti (Figure Six). Ideally one would have performed an ultrasound examination before breeding the mare, but this is not always possible. If the first scan is performed at Day 14 or 15, then it is possible to return the next day in cases of confusion and see if the pregnancy has changed position or grown in size. This should allow differentiation from a cyst before the pregnancies have a chance to become unilaterally fixed. Mares with cysts sometimes are thought to be more likely to have an increased incidence of EED. This could be due to the cyst’s restricting the early movement of the pregnancy. If the pregnancy becomes fixed close to one or several cysts, the cysts might interfere with the absorption of nutrients by the developing pregnancy.
Another advantage of performing the first examination for pregnancy at Day 15 and not Day 18 is that a mare with a shortened luteal phase due to uterine infection can be detected. If examination is delayed until Day 18, it is possible that the mare has ovulated already and the fact that she has had a shortened luteal phase will not be detected. The early pregnancy has a characteristic pattern of growth, and it is important to be familiar with this pattern as any deviation can indicate EED has occurred, or is likely to occur. The following gives you an idea of the stages of growth in the pregnancy within the first 65 days.
- By Day 16:

Fig. 7 – day 16
The early pregnancy is 20 mm in size and normally is fixed at the base of either the left or the right uterine horn. The shape is still regular, but more ovoid than strictly spherical (Figure Seven). The embryo is not yet detectable on ultrasound examination.
- By Day 21:
Fig. 8 – day 21
The conceptus is approximately 28 mm in size and the embryo is approximately 4 mm in length. The embryo normally is first detected on ventral (bottom) surface of the vesicle in a “5 or 6 o’clock” position (Figure Eight). The heartbeat normally can be detected as a rapid flickering movement in the middle of the embryo around this stage of pregnancy. Variation can occur in the location of the embryo. For example, the embryo might first appear high in the dorsal part of the vesicle instead of its more usual site. Such variations in appearance of the image are to be expected and arise due to natural variation or even can be caused by the location of the transducer within the rectum. In some cases, the embryo is first seen in the dorsal sector between 11 o’clock and 1 o’clock and grows downward. These pregnancies often are referred to as “upside down” . Although unusual, there is no evidence this orientation reduces the pregnancy survival rate. They are not an indication of EED. It is important to recognize the embryo and identify a heartbeat because irregular shape of the vesicle is easily confused with an endometrial cyst.
- By Day 30:

Fig. 9 – day 30
The embryo has grown to several millimeters in diameter and is visible on the line separating the pregnancy into two halves (Figure Nine). Allantoic and yolk sacs and the heartbeat clearly can be seen.
- By Day 48:
Fig. 10 – day 45
The fetus has descended approximately two-thirds of the way toward the lower part of the allantois (Figure Ten). The developing umbilical cord is clearly visible.
- By Day 60:
Fig. 11 – day 60
The developing foal has recognizable features such as backbone, chest, head, and stomach (Figure Eleven). Shortly after this – often by day 65 – the diameter of the conceptus exceeds the scanning width of the ultrasound probe. Considerable fetal motility is obvious.




Timing Of Routine Pregnancy Scans
The first scan should be around 15 days after breeding to diagnose pregnancy early and to deal with a twin pregnancy. A second scan around 26 to 30 days after breeding allows your veterinarian to check for normal development of the pregnancy, detect any signs of EED, and confirm that there are no twins. These timings are arbitrary. Extra scans might be needed in mares which are prone to twinning, have many cysts, or have lost pregnancies before. The cost is an important consideration. As with many aspects of horse breeding, a compromise must be struck between what is best and what is practical in economic terms. If a mare only is able to be scanned once on economic grounds, then this should be around Day 28, when an obvious embryo with heart beat should be visible. Mares scanned in foal in the breeding season should be checked in the fall by internal examination to make sure they are still pregnant.
Diagnosis Of EED
Unfortunately, many mares do not return to estrus for a long time following EED due to the continued production of hormones similar to that in a pregnant mare. If the pregnancy is lost at a very early stage, before the maternal recognition of pregnancy, the mare may come back into estrus.
The traditional method of detecting early pregnancy loss has been manual examination of the uterus by palpation via the rectum. However, cases of EED that result in false pregnancy feel very similar to early pregnancy. The only difference is absence of the fetal swelling. This means that it was very difficult to make a reliable diagnosis of EED at an early stage by palpation alone.
As you read earlier, in most situations of EED, the mare continues to produce the same hormones she does if she is pregnant for a long period of time after she has lost the pregnancy. This means that single or even repeated blood samples to measure hormone levels are of limited diagnostic value in cases of suspected EED.
The introduction and development of the use of ultrasonography during the 1980s has proved an invaluable tool in the diagnosis, features, and incidence of EED in the mare. A definitive diagnosis of EED occurs when an embryonic vesicle seen previously is not observed on two consecutive ultrasound examinations. However, it is not necessary to wait until the early pregnancy has completely disappeared as recently it has become apparent that there are many features detectable on ultrasound scan that give us a clue that the mare is at risk for or is in an early stage of undergoing EED.
Ultrasonographic Features Of Early Embryonic Death
Ultrasonographic scanning has provided a valuable tool in studying embryonic death. Because pregnancy is often diagnosed at an early stage, it is important to inform owners that not all pregnancies detected with ultrasound will survive, even in apparently normal mares. There are certain morphological features detected with ultrasound that are typical of mares in which embryonic death is occurring. Some of the consistent features include the following:
- Presence of fluid within the uterine lumen;
- Prominent endometrial edema:
Edema around the vesicle is not unusual to see in normal 15 to 17 day pregnancies. Edema as late as 18 days is unusual and suggests the mare might be returning to estrus. This would be confirmed by visible edema throughout the uterus suggesting that luteal regression has occurred. Failure to visualize a CL in the ovary supports this. The action that should be taken is immediate support of the pregnancy with progesterone in case of luteal regression. Plasma progesterone measurement would confirm the diagnosis, but only retrospectively. Progesterone therapy must be continued until one of the following happens:- Pregnancy failure;
- A new ovulation is detected;
- A normal pregnancy is still present at 100 days, after which placental progesterone will be sufficient for pregnancy maintenance;
- An embryo proper cannot be seen by Day 28.
The advice to the mare owner would be that if luteal regression has occurred, then conceptus loss might follow within the next 24 hours. If the institution of progesterone therapy is in time to prevent loss, then the vesicle might survive. However, because the
- Decreased or prolonged conceptus mobility;
- Undersized or irregularly shaped conceptus;
- Bradycardia or cessation of the embryonic heartbeat;
- Reduced volume of placental fluids;
- Disorganization of placental membranes;
- Hyperechogenic areas in the embryo and membranes;
- Failure of the embryo to appear resulting in a so-called “an-embryonic vesicle”;

Fig. 12 – two CLs!
Examination of the ovaries is important at every examination for pregnancy to provide information on the number and appearance of the CLs. Mares with twins almost always have two corpora lutea (Figure Twelve). The primary CL is visible as a uniformly echoic area on this image. A CL readily detectable on ultrasound usually is producing progesterone. Ultrasonographic assessment of the CL can be useful in assisting a decision to provide exogenous progesterone or progestogen.
Summary:
In conclusion, EED is a major problem to horse breeders. Since we do not know exactly the cause(s), it is difficult to develop a rational treatment program for mares which repeatedly undergo EED. Intensive management (proper feeding, exercise, and avoiding stress) might accomplish the objective of getting a mare to carry a foal to term.
The major advance in recent years has been use of the ultrasound to diagnose EED more readily than was previously possible. This allows the mare to be brought back into estrus and bred again. Hormone treatments with buserelin and progestins also might be useful.
About The Author
Dr Jonathan F Pycock graduated from the Royal Veterinary College, University of London, in 1983 from where he obtained his PhD in 1988 for his thesis on “Breeding Problems in the Mare”. He was then in private equine practice for 6 years working in the UK during their breeding season before heading to the southern hemisphere for their season. In 1994 he took a position as Associate Professor of Equine Reproduction at the University of Utrecht in the Netherlands. Whilst there he developed a special interest in artificial insemination with both chilled and frozen semen and assisted reproductive technologies such as embryo transfer and IVF. He worked extensively in these areas whilst in the Netherlands. He was awarded his Diploma in Equine Stud Medicine in 1994 and in 1995 became an RCVS recognised Specialist in Equine Reproduction. He returned to the UK in January 1997 to begin Equine Reproductive Services, a first opinion and referral private equine practice based in Yorkshire. He has published many papers and several books and book chapters on a variety of equine reproductive topics and recently completed editing the major equine text “Current Therapy in Equine Reproduction”. He has lectured at meetings and given courses all over the world to both veterinary surgeons and breeders. His main interests include ultrasonography, breeding the problem mare and artificial insemination. At the time of publication of this article (2007-9) he was actively involved in researching mechanisms of uterine clearance and what determined susceptibility to endometritis. This was followed by work evaluating the use of oxytocin and depot oxytocin as a post-breeding treatment for mares.